摘要:
目的:分析临床实际中玻璃体腔注射抗新生血管生成因子类药物治疗视网膜静脉阻塞性黄斑水肿的实际状况,并进一步分析其可能原因,以便为临床治疗决策提供进一步的指导。方法:回顾性非随机临床病例研究,共收集研究期间,在我院所有行玻璃体腔注射抗血管内皮生长因子(anti-vascular endothelial growth factor, anti-VEGF)类药物治疗的视网膜静脉阻塞(retinal vein occlusion, RVO)患者61例(62只眼) (去除失访5人)纳入研究,记录患者的年龄、性别、全身病史,注射药物的种类,注射的次数,以及视力情况、黄斑中心凹的厚度改变等;以分析临床治疗中的实际情况。结果:共有男性30例(31只眼)、女性31例(31只眼)纳入研究,平均年龄(58.75 ± 19.30)岁,其中BRVO50例(50只眼),CRVO11例(12只眼);合并有糖尿病等全身疾病的患者比例达56.7%;从患病到就诊的平均时间从6天到2年不等;雷珠单抗注射液与康柏西普注射液的使用频次比为3比1;玻璃体腔注射一次的占45.9%,注射2次及3次的分别占18%及23%,而注射3次以上的为13.1%;黄斑中心凹的平均厚度由治疗前的477.35 ± 202.21微米,降低到随访结束时的259.24 ± 99.52微米,注射治疗后黄斑中心凹的厚度平均减少了218.12微米,差异具有统计学意义。视力由治疗前的平均4.23 ± 0.52提高到随访结束时的平均4.60 ± 0.43,平均提高3行,差异具有统计学意义。除2例在研究期间发生心梗、脑梗外,无新发的眼部及其他全身的并发症。终止治疗原因中,53%由于临床治愈,25%因经济原因放弃治疗,其他原因包括全身心脑血管病发作,高龄等。结论:视网膜静脉阻塞是常见 的眼底疾病,分支静脉阻塞比中央静脉阻塞发病率更高,合并全身疾病的比例高;抗VEGF类药物对视网膜静脉阻塞性黄斑水肿的治疗是有效的,注射治疗后黄斑中心凹的厚度平均减少了218.12微米,视力平均提高3行;注射治疗方案不一,非病情原因影响治疗的最主要原因是经济原因。
Abstract:
Objective: To study the actual state of anti-VEGF drugs in the treatment of macular edema of retinal vein occlusion. Further analyses were also made to provide further guidance for clinical decision. Methods: This is a retrospective nonrandomized clinical case study. A total collection of 62 eyes of 61 patients with macula edema of retinal vein occlusion had been involved in the study (5 patients were excluded to losing the follow-up). The age, the gender, the general disease history, the intra-vitreal injection times and the classes of anti-VEGF drugs were observed. The best corrected visual acuity (BCVA) and the thickness of macular fovea were also observed. Results: A total of 30 males (31 eyes) and 31 females (31 eyes) were included in the study, with an average age (58.75 ± 19.30), of which BRVO50 (50 eyes), CRVO11 (12 eyes); the proportion of patients with systemic diseases such as diabetes was 56.7%. The average time from illness to visit ranged from 6 days to 2 years; and the frequency of using Ranibizumab is three times to that of using Conpercept. The patients with only one intra-vitreal injection were occupied 45.9 percent. Those with two or three injections were occupied 18 and 23 percent. And those with more than three times injections were occupied 13.1 percent. The average of the BCVA was 4.23 ± 0.52 before the treatment, and it was 4.60 ± 0.43 at the end of the follow-up. All patients gained increased BCVA by three lines through operation. There are statistical differences between the BCVA of postoperation and preoperation. The average thickness of the macular fovea was reduced from 477.35 ± 202.21 micrometers to 259.24 ± 99.52 micrometers. And the thickness of macular fovea was decreased by 218.12 micrometer through operation averagely. And there are statistical differences between the thickness of macular fovea of postoperation and preoperation also. In addition to 2 cases of myo-cardial infarction and cerebral infarction during the study, there were no new ophthalmic and other systemic complications. The reason for the termination of the treatment is 53 percent due to clinical recover, 25 percent for economic reasons, and other causes including the onset of cardiovascular disease, and the eldest age, etc. Conclusion: Retinal vein occlusion is a common fundus disease, with a higher incidence of branch vein occlusion than central vein occlusion and a high proportion of systemic diseases. The application of intra-vitreal anti-VEGF injection for the treatment of macula edema of retinal vein occlusion was effective. All patients gained increased BCVA by three lines through operation. And the thickness of macular fovea was decreased by 218.12 micrometer through operation averagely. The treatment protocols were not all the same. The main reason for the unwished termination of treatment was economy.
1. 引言
视网膜分支静脉阻塞(Branch retinal vein occlusion, BRVO)及视网膜中央静脉阻塞(central retinal vein occlusion, CRVO)是继糖尿病性视网膜病变之后最常见的视网膜血管性疾病 [1] [2] ,BRVO的患病率约为0.44%,CRVO的患病率约为0.08%;在世界范围内,约有一千三百九十万BRVO患者及两百五十万CRVO患者 [3] 。静脉阻塞后,由于组织缺氧,导致局部血管内皮生长因子水平上调,引起局部的毛细血管的通透性升高,加上阻塞导致的血管内压力的增大,形成继发性的黄斑水肿,而继发性的黄斑水肿是导致患者视功能损伤最常见的原因。所以目前临床上常用的治疗手段的主要目的就是用各种方法控制黄斑水肿,以期改善视力,包括视网膜激光光凝、玻璃体腔注射糖皮质激素类药物、抗血管内皮生长因子类药物的玻璃体腔注射、玻璃体视网膜手术等治疗方法 [4] - [11] 。其中抗血管内皮生长因子类药物玻璃体腔注射是近年来临床上颇受关注的治疗方法,该类药物通过降低玻璃体腔内血管内皮生长因子的浓度,达到降低病变区毛细血管的通透性、减少渗出、减少新生血管的形成,从而减轻黄斑水肿的作用。由于该类药物的费用较高,需要反复注射,而且局部注射有一定的风险,虽然临床上对其治疗的方案有基本的共识,但是真实世界中,究竟哪种药物更好、需要注射几次,效果是否有差异等问题,目前未见确切的文献报道。除了药物的原因,影响治疗的原因很多,如经济、年龄、全身情况等 [12] - [18] 。本文通过回顾性研究的方法,总结了近4年来我科实际临床工作中应用玻璃体腔注射抗新生血管生成类药物治疗视网膜静脉阻塞导致的黄斑水肿的临床资料,以期通过实际临床工作中的具体情况来试图回答相关的问题,现将结果报告如下。
2. 资料和方法
2.1. 研究对象
回顾性非随机临床病例研究。收集2012年6月1日~2016年6月30日期间、在我院住院救治的、行玻璃体腔注射抗血管内皮生长因子类药物治疗的视网膜分支静脉阻塞、或者视网膜中央静脉阻塞、所导致的黄斑水肿的患者66例(67只眼)的临床资料进行分析研究,随访1年,除去5人失访,纳入研究共61人,62只眼。所有患者均根据临床表现、并经眼底荧光血管造影(fundus fluorescence angiography, FFA)确诊为视网膜分支静脉阻塞、或者视网膜中央静脉阻塞 [19] [20] ,所有患者均经OCT确诊合并有黄斑水肿。所有患者均为本研究进行期间、在我院就诊的、经FFA及OCT确诊的视网膜分支静脉阻塞、或者视网膜中央静脉阻塞合并黄斑水肿(注射治疗的具体标准为:黄斑中心凹厚度 ≥ 250微米,或者局部视网膜神经上皮层间有明显的囊腔)的患者;既往有青光眼、视力低下病史,半年内发生过心脑血管疾病、屈光介质混浊影响眼底观察、及个人不愿意接受玻璃体注射治疗的患者除外。所有患者在接受玻璃体腔注射抗血管内皮生长因子药物治疗之前、均按程序通过医院伦理委员会的批准,并签署知情同意书。
2.2. 方法
采用回顾性非随机临床病例研究的方法。
2.2.1. 随访时间
明确诊断后,患者同意治疗时起、到最后一次玻璃体注射治疗后1年止、为治疗随访区间。玻璃体注射治疗后,每月随访,按病情需要决定是否再次注射;病情稳定后,延长随访时间,如果病情有变化及时随访复查;病情稳定达半年者,注射后半年及一年各随访一次。
2.2.2. 观察指标
所有入组的患者统计一般情况,包括年龄、性别、全身病史,注射的药物,注射的次数等;记录每个观察点的最佳矫正视力(best corrected visual acuity, BCVA),视力均采用LogMAR视力记录;黄斑OCT检查;眼压、裂隙灯显微镜、间接检眼镜、眼底照相等。对于1年以上未继续治疗或复查就诊的病人,调查及分析其原因。
2.2.3. 注射方法
所有患者在接受玻璃体腔注射药物之前3天、开始双眼点左氧氟沙星滴眼液4次/日,术前15分钟盐酸奥布卡因滴眼液点眼3次,在无菌手术室按内眼手术进行消毒铺巾,先后用5 g/L的聚维酮碘溶液及生理盐水冲洗结膜囊,以TB针抽取0.05 ml (0.5 mg)的药液,在颞上象限角膜缘后4 mm经睫状体平坦部垂直于眼球壁向眼球中心方向进针,经瞳孔确认注射器针头位于玻璃体腔的情况下,将药液缓慢注射于玻璃体腔内,出针后用无菌干棉签按压注射点30秒,确认无出血及其他不良现象后,结膜囊涂妥布霉素地塞米松眼膏后用无菌纱布遮盖术眼。术后次日去除术眼纱布,继续点左氧氟沙星滴眼液4次/日共3天 [21] 。并嘱咐患者按月及按要求定期复查随访。复查时根据患者的主观症状及OCT结果,决定是否再次行玻璃体腔注射治疗(主观视力明显下降,或者黄斑中心凹厚度增加 ≥ 100微米者,建议并再次行注射治疗,否则就继续观察随访)。玻璃体腔注射药物的种类主要是根据医生介绍后患者及其家属的意愿决定。我院使用的抗血管内皮细胞生长因子类药物共两种:分别是美国Genentech公司生产的雷珠单抗眼用注射液和成都康弘生物科技有限公司生产的康柏西普眼用注射液。
2.3. 统计处理
应用SPSS19.0对数据进行统计处理,对于从患病到就诊的平均时间的比较采用经非参数检验M-WU检验,对于视力、黄斑区视网膜神经纤维层厚度的比较采用配对样本t检验,以0.05作为检验标准,小于0.05表示有统计学意义。对于其他指标都采用描述性统计。
3. 结果
3.1. 研究对象的一般情况
所有患者中,男性30例(31只眼),女性31例(31只眼);年龄20~90 (58.75 ± 19.30)岁。诊断BRVO50例(51只眼),诊断CRVO11例(11只眼)。合并有高血压、糖尿病、高血脂这三种情况之一的患者比例达56.7%。年龄、性别在RVO中无显著性差异。
3.2. 从患病到就诊的平均时间
从6天到2年不等,BRVO患者从患病到就诊的中位数时间是31.76天,CRVO患者从患病到就诊的中位数时间是21.40天。经非参数检验M-W U检验,P值 = 0.081,中位数比较差异无显著性。
3.3. 注射药物的种类情况及注射次数
我院抗VEGF药物共两种,分别是雷珠单抗眼用注射液(美国Genentech生产)和康柏西普眼用注射液(成都康弘生物科技有限公司生产)。两种药物的使用频次是45比16。只注射1次的为28人,占45.9%;注射2次的为11人,占18.0%;注射3次的为14人,占23.0%;注射4次及以上的为8人,占13.1%;其中一位CRVO的患者,其注射次数已经达36次,目前仍然在治疗中。
3.4. 初诊及随访结束时视力情况
初诊时视力平均为4.23 ± 0.52,随访结束时视力平均为4.60 ± 0.43,所有患者治疗后视力平均提高0.38 ± 0.38,经配对t检验,t值为6.174,P值为0.000,差异有统计学意义。
3.5. 黄斑OCT厚度改善情况
初诊时黄斑中心凹的平均厚度为477.35 ± 202.21微米,随访结束时黄斑中心凹的平均厚度为259.24 ± 99.52微米,所有患者治疗后黄斑中心凹的平均厚度减少了218.12 ± 179.55微米,经过配对t检验,(不分BRVO和CRVO组),t值 = 8.239,P值 = 0.000,差异有统计学意义。
3.6. 并发症情况
所有患者,治疗过程中未出现新发生的并发性白内障;未出现明显的眼压升高的情况;无感染性眼内炎或者无菌性眼内炎的发生;未发生任何种类的视网膜脱离及视网膜出血。2例因出现心梗、脑梗等心脑血管并发症终止治疗。
3.7. 终止治疗的原因
如图1,终止治疗后1年以上的原因中,53%因临床治愈,其中视力恢复4.9以上为16例17只眼(15例15眼BRVO,1例2眼CRVO),占28%。其次为经济原因放弃治疗;其他(转院、中医等)、继续治疗有7%,还有高龄、心脑血管并发症等原因。
4. 讨论
视网膜分支静脉阻塞及视网膜中央静脉阻塞是继糖尿病性视网膜病变之后最常见的视网膜血管性疾病。由于视网膜静脉回流障碍导致视网膜出血、水肿及无灌注区的形成,患者视力不同程度下降。视网膜的缺氧诱发局部VEGF表达增加、与黄斑水肿的发生有明确的关系。使得玻璃体腔内注射抗VEGF药物,成为治疗静脉阻塞性黄斑水肿的一种治疗手段 [1] [2] [3] [4] 。
基于疾病本身的特点及抗VEGF药物费用较高、需反复注射、有一定的风险等因素的存在 [14] [15] [16] [17] [18] ,导致了临床工作中对该类疾病治疗过程的个体差异性。本研究发现,RVO以中老年多见,
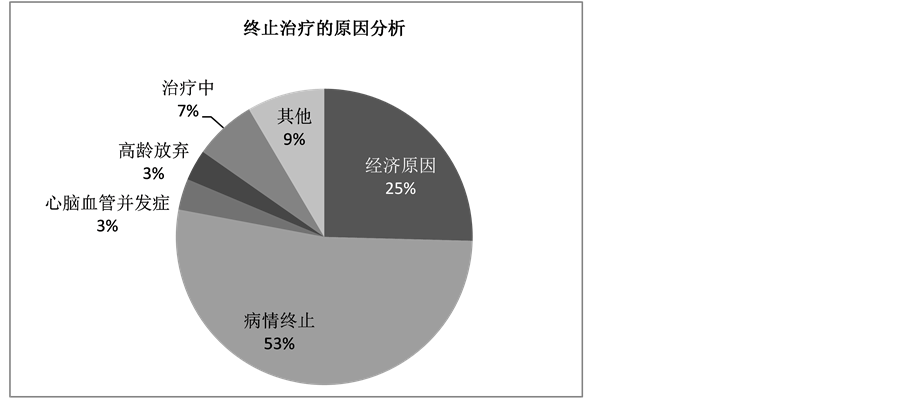
Figure 1. Reasons for termination of treatment
图1. 终止玻璃体注射治疗的原因
性别之间无明显的差异,合并高血压、糖尿病等全身情况的比例较高,与文献结果相符 [1] [2] [3] 。从患病到就诊的中位数时间BRVO患者是31.76天,而CRVO患者为21.40天,考虑可能与CRVO患者视网膜病变范围更广、病情更重、视力影响更大有一定的关系。而雷珠单抗与康柏西普的使用频次比为3比1,这可能与前者进入临床时间更早、患者对进口药物的倾向性有关。在注射次数方面,只注射一次的占4成半,注射2次及3次的分别占18%及23%,而3次以上的为13%左右,这一方面可能受治疗的投入与产出比太高影响,另一方面可能受治疗的反复性及病情本身特点的影响。
视网膜静脉阻塞是常见而严重的眼底疾病,尽管抗VEGF药物需反复注射、费用较高,但是经过治疗,患者的黄斑中心凹的水肿能够平均减少了218.12微米、视力能够平均提高3行,而且没有明显的局部及全身的并发症,这与文献的报道也是相符的 [22] [23] [24] [25] 。所以抗VEGF药物对于视网膜静脉阻塞性黄斑水肿的治疗是有益的。
尽管如此,临床实践中并非所有病人能完成治疗。终止治疗后继续随访1年以上的数据显示,超过一半的病人是因为临床治愈而无需治疗,而47%仍需要继续治疗,其中只有7%的病人能够坚持玻璃体腔注射治疗。最重要原因是经济负担重,其中以农村及低收入人群为主,CRVO多于BRVO;其次,当告知病人,治疗可能需要3年,10万块钱,而预后视力低于期望值时,尽管1次治疗获益很大,病人最终也因为经济原因选择放弃治疗。放弃玻璃体腔注射抗VEGF类药物治疗后,半数病人辅助激光或中药治疗。
总之,视网膜静脉阻塞是常见的眼底疾病,其导致的黄斑水肿是影响视力的重要原因。目前临床上常常采用包括玻璃体腔注射抗VEGF药物、激光光凝、玻璃体腔注射曲安耐得、玻璃体手术、中医中药等手段在内的多种治疗手段,而且倾向于这些治疗手段的联合运用。联合治疗可能起到互补或协同作用,且联合治疗可减少并发症的机会 [1] [3] [5] [9] [10] [11] [25] 。由于本研究系回顾性研究、样本数量有限、有少部分患者的观察随访时间较短,所得结论恐有偏差。这还需要大样本、多中心的随机双盲对照研究结果的证实。
5. 结论
视网膜静脉阻塞是常见的严重的眼底疾病;视网膜分支静脉阻塞比视网膜中央静脉阻塞的发病率更高;合并全身疾病的比例较高。抗VEGF类药物对视网膜静脉阻塞性黄斑水肿的治疗是有效的。玻璃体注射抗VEGF类药物后、黄斑中心凹的厚度平均减少了218.12微米,视力平均提高3行,差异有统计学意义。临床实际中,注射治疗方案不一,非病情原因影响治疗的最主要原因是经济原因。
基金项目
国家自然科学基金面上项目(81271016),首都特色基金项目(Z141107002514056)。