摘要: 患者,男,64岁,20余天前无明显诱因出现腹痛,呕吐,上腹部剑突下及右上腹部为重;腹部触诊:腹软,上腹部触及一直径约8 cm左右包块,边界不清,无压痛、无反跳痛;CT平扫 + 增强显示:胰腺体尾部显示不清,其走行区见团块状软组织密度影,边界不清并局部与邻近胃壁分界不清,大小约6.8 cm × 9.0 cm × 8.3 cm,密度欠均匀,平均CT值约35 HU,增强扫描呈不均匀强化,各期CT值分别为51 HU、69 HU、73 HU,内见多发低、稍低密度强化减低区;CT诊断:考虑恶性肿瘤性病变(胰腺来源可能性大);患者局麻下行超声引导下胰腺包块穿刺活检术,病理诊断:考虑为(胰腺) Ewing肉瘤/原始神经外胚层肿瘤(PNET)。
Abstract:
The patient, a 64-year-old male, had abdominal pain and vomiting more than 20 days ago without obvious inducement, and heavier weight in the inferior xiphoid process and the right upper abdo-men. Abdominal palpation: the abdomen is soft, the upper abdomen touches a lump about 8 cm in diameter, the boundary is unclear, no tenderness, no rebound pain; CT plain scan + enhanced dis-play: The pancreatic body and tail were not clearly displayed, and clumpy soft tissue density shad-ows were seen in the walking area, with unclear boundaries and unclear local boundaries with the adjacent gastric wall. The size was about 6.8 cm × 9.0 cm × 8.3 cm, and the density was not uniform. The average CT value was about 35 HU, and the enhancement scan showed uneven enhancement, and the CT value of each stage was 51 HU, 69 HU, 73 HU, respectively. Multiple low and slightly low density enhancement reduction areas were observed; CT diagnosis: Malignant neoplastic lesions (pancreatic origin is more likely) were considered. The patient underwent ultrasound-guided pan-creatic mass biopsy under local anesthesia. Pathological diagnosis was considered as Ewing sarcoma (pancreas)/primitive neuroectodermal tumor (PNET).
1. 临床资料
患者,男,64岁,20余天前无明显诱因出现腹痛,呕吐,上腹部剑突下及右上腹部为重,疼痛不向他处放射,与进食无明显相关;10余天前呕吐、疼痛加重,于外院行上腹部CT检查提示上腹部软组织肿块,其内密度不均,性质及来源待定,于2023年6月11日收治入院;腹部触诊:腹软,上腹部触及一直径约8 cm左右包块,边界不清,无压痛、无反跳痛;
入院时查体:T:36℃,P:72次/分,R:20次/分,BP:152/92 mmHg。营养差。全身浅表淋巴结未触及肿大。双肺触觉语颤对称,无胸膜摩擦感,叩诊音清,听诊呼吸音正常,未闻及干湿啰音,无胸膜摩擦音。心率齐,各瓣膜区未闻及病理性杂音。腹软,上腹部可触及一直经约8 cm左右包块,边界不清,无压痛、反跳痛,肝脾肋下未触及,Murphy(−),移动性浊音阴性,肠鸣音正常、4次/分,双下肢无水肿。
CT平扫 + 增强显示:胰腺体尾部显示不清,其走行区见团块状软组织密度影,边界不清并局部与邻近胃壁分界不清,大小约6.8 cm × 9.0 cm × 8.3 cm,密度前均匀,平均CT值约35 HU,增强扫描呈不均匀强化,各期CT值分别为51 HU、69 HU、73 HU,内见多发低、稍低密度强化减低区,病变以胰尾部萎缩并胰管扩张(图1)。
超声引导下胰腺包块穿刺活检术:患者取平卧位,超声引导下穿刺点定位于上腹区,常规消毒铺巾,2%利多卡因4 ml局部浸润麻醉,以18G活检针穿刺进入胰腺包块内取材,共进针3次,进针深度约1.0 cm,取得组织条长度0.5 cm,取材送检,伤口消毒加压包扎,术毕,给予静脉推注白眉蛇毒血凝酶注射液1单位,术中术后患者无特殊不适,安返。病理诊断:(胰腺)送检穿刺组织内见小圆细胞肿瘤,结合免疫组化,考虑为Ewing肉瘤/原始神经外胚层肿瘤(PNET)。免疫组化:CK(−)、Vimentin(+)、FLi-1(+)、CD99(+)、NKX2.2少数(+)、CD10(−)、CgA(−)、β-catenin(−)、TFE-3部分弱(+)、E-cadherin(−)、CylinD1部分(+)、ERG点灶(+)、ER(−)、PR(−)、INSM1(−)、S-100(−)、PGP9.5(−)、NSE(−)、Ki-67指数约90%。
 (a)
(a)  (b)
(b) 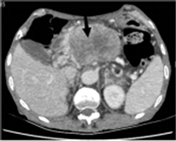 (c)
(c)  (d)
(d)
Figure 1. (a), (b) and (c) are CT plain scan and enhanced images, and the black arrows in the figure indicate the lesion area. (d) is the hematoxylin-Y staining ×4 image
图1. (a)、(b)、(c)为CT平扫及增强图像,图中黑色箭头所指为病灶区;(d)为苏木素–伊染色×4图像
2. 讨论
尤因肉瘤/原始神经外胚层肿瘤(Ewingsarcoma/Primitive Neuro-Ectodermal Tumors, EWS/PNET)隶属于EWS家族肿瘤(Ewing sarcoma family tumor, ESFT),包括骨EWS、骨外EWS、PNET和Askin瘤。EWS/PNET在各个年龄阶段均可发病,在<5岁和>35岁的人群中发病率较高 [1] 。骨外EWS/PNET以椎旁和胸椎软组织多见,文献报道亦可见于食管、胰腺、回肠、肾脏、膀胱、阴道、子宫、阴茎、肾上腺、乳腺和颅内组织 [2] 。文献报道胰腺EES大多数发生在胰腺头部,因发育成胰腺头部的原始神经上皮干细胞与形成胰腺体和尾部的原始神经干细胞不同 [3] 。
本例病例中,患者为中年男性,病灶发生在上腹部,病程较短,发现病灶20余天,近10天症状进行性加重,病灶是位于上腹部剑突下的实性肿块,关于胰腺尤文肉瘤/原始神经外胚层肿瘤的相关影像报道十分少见,本例病案中,患者的CT影像表现主要为:胰腺走行区内团块状软组织密度影,边界与周围胃壁分界不清,密度欠均匀;增强扫描为不均强化,内见多发低、稍低密度强化减低区,总体临床表现和影像表现考虑为胰腺尤文肉瘤/原始神经外胚层肿瘤。
临床和放射学鉴别诊断包括其他更常见的原发性胰腺肿瘤,如外分泌腺癌,以及原发性腹膜后肿瘤。由于MRI、CT或US的影像学表现是非特异性的,因此通过开放活检或影像引导下粗针活检进行组织取样对于明确诊断至关重要 [4] 。
目前,在北美和欧洲,尤因肉瘤的一般治疗策略采用多药诱导化疗,然后对原发肿瘤进行局部治疗,进行额外的化疗,并在可行的情况下对所有转移部位进行巩固局部治疗。两种方法的差异包括独特的诱导化疗方案,欧洲越来越多地使用联合治疗进行原发性肿瘤控制,以及根据预后因素和组织学反应的辅助化疗差异更大,包括在欧洲方案中更常见的高剂量化疗和干细胞挽救。儿童肿瘤学组和国际小儿肿瘤学会的重点是通过增加联合治疗的使用、强化放疗或识别新型全身性药物,确定哪些患者可以从加强局部控制中受益 [5] 。
鉴别诊断:尤因肉瘤/原始神经外胚层肿瘤的鉴别诊断包括1) 神经母细胞瘤:CT上,肿块通常为等密度或轻微低密度,囊性变性和坏死区密度低,对比增强扫描可轻度至显著增强,但囊性变性和坏死区无增强 [6] ;2) 横纹肌肉瘤:动脉期可以看到外周环状不均匀增强,从静脉期和延迟期可以看到逐渐的中心性不均匀增强 [7] ;3) 胰腺神经内分泌肿瘤:典型的神经内分泌肿瘤平扫呈低密度,增强扫描动脉期明显强化,静脉期、延迟期持续强化,部分病灶略减退,可以发生囊变坏死 [8] ;4) 胰母细胞瘤 [9] ,胰母细胞瘤平扫低密度,增强后不均匀强化,其内可见无强化低密度区;可见钙化,约33%的肿瘤CT显示有钙化存在;肿瘤有完整或不完整包膜,侵犯周围血管及脏器,也可转移至网膜及颈部淋巴结,直接侵犯至门静脉及分支 [10] [11] 。
3. 总结
综上所述,胰腺尤因肉瘤/原始神经外胚层肿瘤是一种十分罕见的恶性肿瘤,描述这些肿瘤的报道十分有限,胰腺受累极其罕见,占原发肿瘤的0.3% [12] ,发病时间较短,起病隐匿,症状也因人而异。常用的影像诊断方法包括腹部CT和磁共振成像,但目前缺少特异的影像学诊断将其与其他胰腺恶性肿瘤鉴别。手术切除后放化疗是最广泛接受的选择,但目前还没有最佳治疗方案,患者预后较差。
声明
该病例报道已获得病人知情同意。
NOTES
*通讯作者。