摘要: 目的:探讨极低出生体重儿发生代谢性骨病的预测指标。方法:选取确诊代谢性骨病的129例极低出生体重儿设为病例组;同期47例非代谢性骨病极低出生体重儿为对照组。分析比较两组新生儿出生时血清钙、血磷、血钙磷乘积、血碱性磷酸酶等。结果:出院后确诊代谢性骨病的极低出生体重儿出生时平均血清钙、血磷、血钙磷乘积与对照组无统计学差异(P值分别为0.574、0.360、0.325);血碱性磷酸酶水平低于对照组,差异有统计学意义(P = 0.017);使用ROC曲线分析,血碱性磷酸酶曲线下面积为0.519;血碱性磷酸酶(241.5 U/L)对代谢性骨病的预测敏感性为84.5%,特异性为31.9%,95%CI:0.413~0.624。结论:MBDP极低出生体重儿出生时血碱性磷酸酶可能存在差异,但无助于预测代谢性骨病的发生。
Abstract:
Objective: To investigate the predictors of metabolic bone disease in very low birth weight infants. Methods: 129 very low birth weight infants diagnosed with metabolic bone disease were selected as the case group; 47 very low birth weight infants with non-metabolic bone disease during the same period were selected as the control group. The serum calcium, serum phosphorus, serum calcium and phosphorus product, and serum alkaline phosphatase at birth were analyzed and compared between the two groups of infants. Results: The mean serum calcium, serum phosphorus, and se-rum calcium and phosphorus product of very low birth weight infants diagnosed with metabolic bone disease after discharge were not significantly different from those in the control group (P values were 0.574, 0.360, and 0.325, respectively); The enzyme level of serum alkaline phosphate was lower than the control group, and the difference was statistically significant (P = 0.017). Using ROC curve analysis, the area under the curve of serum alkaline phosphatase was 0.519; The sensitivity of serum alkaline phosphatase (241.5 U/L) for the prediction of metabolic bone disease was 84.5%, the specificity was 31.9%, 95%CI: 0.413~0.624. Conclusions: There may be differences in serum alkaline phosphatase at birth in very low birth weight infants with MBDP, but they are not helpful in predicting the occurrence of metabolic bone disease.
1. 引言
早产儿代谢性骨病(metabolic bone disease of prematurity, MBDP),也称为早产骨量减少或佝偻病,是一种以骨矿物质含量降低,类骨质矿化不足为特征的疾病 [1] 。是由于机体内钙磷代谢紊乱及有机蛋白质基质含量减少或骨代谢紊乱所致的全身性骨骼疾病,是多种营养和生物力学因素的共同结果 [2] 。其本质是早产儿骨矿物质含量未能满足正常生长发育所需,常伴有低磷血症、高碱性磷酸酶血症等血生化和骨骼矿化不足的影像学表现 [1] [2] 。MBDP未及时诊治,可导致早产儿骨骼脆弱性增加,随着疾病进展,近期常伴随宫外生长发育迟缓。呼吸机依赖等;远期则可能观察到佝偻病改变、骨矿物质含量降低、易罹患骨质疏松甚至骨折等不良后果 [3] [4] 。在疾病发展至远期表现时,MBD早产儿很少出现明显症状 [3] [4] [5] ,因此筛查和诊断手段尤为重要。国内外建议新生儿筛查时出现低磷、血清ALP升高等生化可考虑MBD [5] 。
1) 研究对象
广州市妇女儿童医疗中心及东莞市妇幼保健院2所医院2020年9月1日至2021年3月31日新生儿科住院的极低出生体质量(very low birth wt, VLBW)新生儿为研究对象,将确诊代谢性骨病的129例极低出生体重儿设为病例组;同期47例非代谢性骨病极低出生体重儿为对照组进行回顾性分析。本研究全部调查对象均获得家属同意并签署书面知情同意书。
2) 纳入标准
① 出生后即刻入院;② 早产,即出生胎龄 < 37周;③ 出生体质量 < 1500 g;④ 住院时间 > 2周。
3) 排除标准
排除有先天性遗传代谢病、青紫型先天性心脏病、先天性胃肠道畸形,新生儿期行各种外科手术治疗者。
4) 诊断标准
出生3周后血碱性磷酸酶(alkaline phos-phatase, ALP) > 900 IU/L血PTH > 180 pg/mL,伴有血磷 < 1.5 mmol/L。X线片有长骨末端骨质稀疏、干骺端杯口样或毛刺样改变,肋骨末端膨大,骨膜下新骨形成或骨折等表现。以及定量超声法提示骨量减少<40%的骨质疏松 [1] [2] 。
5) 检测项目
将病例组及对照组的胎龄(天数)、出生体重(kg)、出生头围(cm)、出生身长(cm)、出生时血液学监测数值包括血清磷(umol/L)、血清钙(umol/L)、血碱性磷酸酶(U/L)等进行记录分析。
6) 统计分析
使用采用SPSS22.5软件进行分析,计量资料用(x±s)表示,使用t检验。计数资料使用c2检验,判断标准为P < 0.05。通过受试者工作特性(receiver operating characteristic, ROC)曲线分析检测数值对极低出生体重儿代谢性骨病的敏感性及特异性。
2. 结果
2.1. 研究对象基本特征
整个研究过程共收集129例MBDP病例和47名对照组。所有研究对象的性别比(男:女)为1.17 (95/81),病例组性别比为1.0 (67/62),正常病例性别比为1.5 (28/19),两组研究对象无统计学意义上的性别比差异(c2 = 0.809, P = 0.369)。两组资料基本特征中出生体重、出生身长、出生头围均无统计学差异,胎龄(天数)比较差异有统计学差异(t值为5.293,P = 0.000),见表1。

Table 1. Basic characteristics of two groups of data
表1. 两组资料的基本特征
2.2. 两组血清检测值分析
如表2所示:两组资料血清检测中血清钙、血清磷、血磷血钙乘积均无统计学差异(P > 0.05)。血碱性磷酸酶病例组低于对照组,差异有统计学意义(t值为−0.2473,P = 0.017)。
Table 2. Analysis of serum test values of two groups
表2. 两组血清检测值分析
2.3. 血清碱性磷酸酶的ROC曲线
病例组血清碱性磷酸酶与对照组相比,差异有统计学意义(P < 0.05),曲线下面积为0.519;极低出生体重儿血碱性磷酸酶(241.5U/L)对代谢性骨病的预测敏感性为84.5%,特异性为31.9%,95%CI:0.413~0.624,如图1。
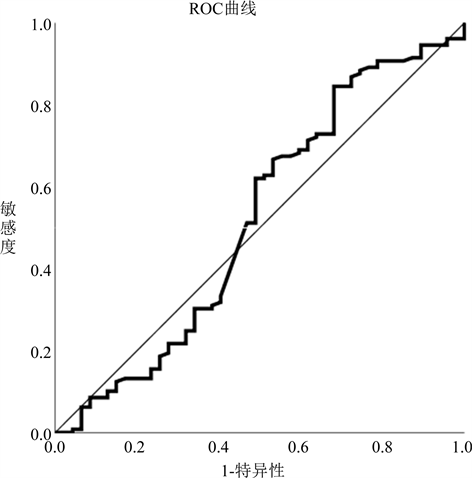
Figure 1. ROC curve of serum alkaline phosphatase for metabolic bone disease prediction
图1. 血碱性磷酸酶对于代谢性骨病预测的ROC曲线
3. 讨论
MBDP主要的生化变化包括血清磷水平降低,血磷浓度可较好反映骨磷储备状况。低磷血症是钙磷代谢紊乱的早期生化表现,一般在生后1~2周内可检测。血磷持续降低提示磷摄入不足和骨质疏松的风险增加 [6] 。这可能是由于磷酸盐缺乏或PTH水平升高。磷酸盐缺乏会增加骨化三醇的合成,并可能导致高钙血症,从而抑制PTH水平 [7] 。此外,肾脏对磷酸盐的再吸收增加,因此,肾小管对磷酸盐的再吸收也是衡量磷酸盐稳态的有效手段。但因为血磷特异度较高,敏感度较低 [6] ,血磷 < 1.8 mmol/L提示低骨密度的特异度为96%,但灵敏度仅为50%,在早期诊断方面价值欠缺 [1] [2] [8] 。本研究提示血磷对预测极低出生体重儿发生代谢性骨病方面无统计差异。
碱性磷酸酶(alkaline phos-phatase, ALP)为糖蛋白酶,由多种组织分泌产生,至少有4种同工酶。作为成熟成骨细胞的活性标志物可反映骨代谢情况。新生儿体内90% ALP来源于骨骼,一般在生后14至21天内呈生理性轻度升高。一般认为血钙磷降低伴ALP升高才考虑MBDP。
目前关于ALP是作为MBDP的诊断指标方面,各研究结果不尽相同。Hung [9] 等发现胎龄 < 34周早产儿诊断MBDP,建议血ALP > 700 IU/L的诊断敏感度为73%,特异度为74%。Viswanathan等 [10] 以及Igueras-Aloy等 [11] 研究显示,ALP > 500 IU/L与MBDP相关。F. Backström等 [12] 发现,根据DEXA检查结果,ALP > 900 IU/L伴有血磷 < 1.8 mmol/L诊断MBDP的灵敏度和特异度分别达100%和71%。ALP水平的增高与MBDP的发生相关,可早于临床症状的出现 [13] 。
血清碱性磷酸酶水平 ≥ 900 IU/L对MBD有100%的敏感性和70%的特异性,ALP浓度在MBD中可能增加五倍 [1] [4] 。Viswanathan等人 [4] [10] 发现ELBW婴儿的ALP在第2个月达到高峰。此外ALP容易受到胆汁淤积症、感染、铜缺乏、锌缺乏以及应用糖皮质激素等因素影响 [14] [15] 。因此在ALP升高考虑诊断MBDP时应谨慎,因为肝脏或胃肠道疾病也可导致其升高 [1] [4] ,国内早产儿代谢性骨病临床管理专家共识推荐血碱性磷酸酶 > 900 IU/L,伴有血磷 < 1.8 mmol/L高度提示MBDP。出生3周后血PTH > 180 pg/mL,伴有血磷 < 1.5 mmol/L,提示严重MBDP。本研究显示,极低出生体重儿血碱性磷酸酶水平低于对照组,差异有统计学意义(P = 0.017);使用ROC曲线分析,血碱性磷酸酶曲线下面积为0.519;血碱性磷酸酶(241.5 U/L)对代谢性骨病的预测敏感性为84.5%,特异性为31.9%,95%CI:0.413~0.624。因此MBDP极低出生体重儿与正常极低出生体重儿出生时血碱性磷酸酶可能存在差异,但可能无法用于预测代谢性骨病的发生。
此外有研究显示甲状旁腺激素相较于ALP和血磷在早期筛查MBDP方面更敏感 [16] 。PTH水平在诊断MBD方面比ALP有更好的特异性。三周时PTH水平 > 180 pg/mL或磷酸盐浓度 < 4.6 mg/dL。产后诊断重度MBD的敏感性为100%,特异性为94%。本研究暂未检测甲状旁腺激素。
本研究作为回顾性研究可能存在选择性偏倚,此外采用检验方法中自变量与因变量可能存在其它因素干扰未能考虑进去,且作为双中心研究例数不大,因此具有一定局限性。今后期望通过前瞻性、大样本的研究进一步探讨血碱性磷酸酶在代谢性骨病的预测及结局改善中的价值。
基金项目
广州市合生元营养与护理研究院“母婴临床研究专项基金”项目。
参考文献