摘要: 目的:探讨各项超声征象在诊断Caroli病中的应用价值。资料与方法:回顾性分析2003年1月~2021年12月于我院就诊的15例Caroli病的超声图像及临床资料,所有病例均经肝穿刺活检组织学或增强CT证实。观察并记录声像图是否存在肝内囊性病变,囊性病变内是否出现“中心圆点征”、“桥征”、“串珠征”、“囊尾征”以及高频线阵探头模式下肝内囊性病变与肝内胆管壁是否存在连续性。结果:①14例超声图像见肝内囊性病变;②单独以腹部低频探头观察到“中心圆点征”、“桥征”、“串珠征”、“囊尾征”作为诊断征象,诊断CD分别为5例、5例、4例、6例,诊断符合率分别为33.3%、33.3%、26.7%、46.7%;单独以高频线阵探头观察到肝内囊性病变与肝内胆管相连续作为诊断征象,诊断CD为11例,诊断符合率为73.3%,与上述征象诊断符合率比较,差异均有统计学意义(P均<0.05)。结论:高频线阵探头观察到肝内囊性病变与肝内胆管相连续是Caroli病最重要的超声诊断征象,超声诊断符合率为73.3%。
Abstract:
Purpose: To investigate the application value of various ultrasonic signs in diagnosis of Caroli dis-ease. Materials and Methods: Ultrasound images and clinical data of 15 patients with Caroli disease admitted to our hospital from January 2003 to December 2021 were retrospectively analyzed. All cases were confirmed by liver biopsy histology or enhanced CT. The ultrasonography was observed and recorded whether there were intrahepatic cystic lesions, whether there were “central dot sign”, “bridge sign”, “beaded sign” and “caudal sign” in the cystic lesions, and whether there was continui-ty between intrahepatic cystic lesions and intrahepatic bile duct wall under high- frequency linear array probe mode. Results: ① Hepatic cystic lesions were observed in 14 cases. ② “Central dot sign”, “bridge sign”, “beaded sign”, and “caudal sign” were observed as diagnostic signs by low-frequency abdominal probes alone, CD was diagnosed in 5, 5, 4 and 6 cases, respectively, and the coincidence rates were 33.3%, 33.3%, 26.7% and 46.7%, respectively. Continuous intrahepatic cystic lesions and intrahepatic bile duct were observed separately by high-frequency linear array probe as diag-nostic signs, CD was diagnosed in 11 cases, and the diagnostic coincidence rate was 73.3%. The dif-ferences were statistically significant compared with the diagnosis coincidence rate of the above signs (P < 0.05). Conclusion: Continuous intrahepatic cystic lesion and intrahepatic bile duct ob-served by high-frequency linear array probe is the most important ultrasonic diagnosis sign of CD, and the coincidence rate of ultrasonic diagnosis is 73.3%.
1. 引言
Caroli病(Caroli Disease, CD)全称为交通性海绵状肝内胆管囊状扩张症,是一种常染色体隐性遗传病 [1] 。由于发病率低,起病隐匿,超声医生对其往往缺乏足够的认识,甚至将肝内胆管的囊性扩张误认为肝囊肿,导致误诊漏诊 [2] ,而未经干预的CD预后不佳,部分患者进展为肝硬化、门脉高压 [3] [4] ,甚至7% CD患者最终发展为恶性肿瘤,其发生风险是正常人群的100倍 [5] 。本研究拟对我院15例CD患者的超声影像和临床资料进行回顾性分析,探讨各项超声征象诊断Caroli病的应用价值,以期早期发现CD,改善患者的预后。
2. 资料与方法
2.1. 研究对象
回顾性分析2003年1月~2021年12月于我院就诊的15例Caroli病患者的临床及超声资料。男性9例,女性6例,男女比例3:2,年龄16~32岁,平均年龄(23.5 ± 6.8)岁。纳入标准:①经肝穿刺活检组织学或增强CT证实为Caroli病;②肝活组织学或影像学检查排除原发性胆汁性胆管炎、原发性硬化性胆管炎等胆管疾病;③留存有腹部凸阵探头和高频线阵探头两种模式下的超声图像。本研究方案经由医院伦理委员会审批,患者均签署知情同意。
2.2. 仪器与方法
使用美国GE Logiq E8和法国Supersonic Aixplorer彩色多普勒超声诊断仪,腹部凸阵探头和和高频线阵探头,频率分别为3~5 MHz和5~12 MHz。
回顾分析所有研究对象的超声图像,观察是否存在肝内囊性本病,记录囊性病变大小和形态,记录是否存在肝脏弥漫性病变、肝内外胆管及胆囊结石、胆道扩张及腹部其他脏器病变情况,记录腹部低频探头模式下肝内囊性病变是否出现“中心圆点征”、“桥征”、“串珠征”、“囊尾征”,高频线阵探头模式下是否观察到肝内囊性病变与肝内胆管相连续。
2.3. 统计学分析
应用SPSS 18.0行数据分析。计量资料以均数 ± 标准差(
± s)表示,计数变量以例数(构成比)表示;各项征象超声诊断符合率之间的比较采用Fisher确切概率法,以P < 0.05为差异有统计学意义。
3. 结果
3.1. 一般资料
首发疾病中,不明原因肝硬化5例,肝内胆管结石2例,胆囊结石2例,海绵肾1例,黄疸1例,无症状4例(见表1)。15例患者中,10例经肝组织学、5例经增强CT证实为Caroli病。

Table 1. Primary disease in 15 patients with Caroli’s disease
表1. 15例Caroli病患者首发疾病
3.2. 超声表现
14例超声图像见肝内囊性病变。单独以腹部低频探头观察到“中心圆点征”、“桥征”(图1)、“串珠征”(图2)、“囊尾征”作为诊断征象,诊断CD分别为5例、5例、4例、6例,诊断符合率分别为33.3%、33.3%、26.7%、46.7%;单独以高频线阵探头观察到肝内囊性病变与肝内胆管相连续(图3)作为诊断征象,诊断CD为11例,诊断符合率为73.3%,与上述征象诊断符合率比较,差异均有统计学意义(P均<0.05);误诊2例:1例因囊性病变位于声像图远场高频探头无法探及,超声诊断单纯肝囊肿;1例肝内囊性病变较小(平均直径1.0 mm),位于膈顶,囊肿内部及与周围胆管连续情况观察不满意,超声诊断为单纯肝囊肿;漏诊1例:患者超声仅见肝内胆管树枝状扩张,最宽处3 mm,超声诊断肝内胆管扩张;(见表2)。
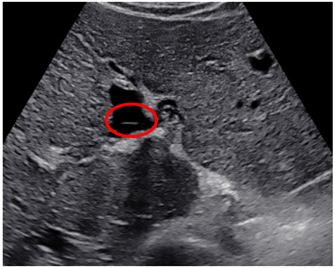
Figure 1. Bridge sign. Ultrasound signs of Caroli’s disease (red circle)
图1. 桥征。Caroli病超声征象(红圈)
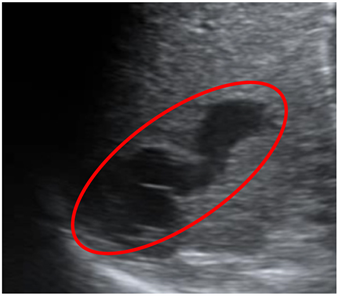
Figure 2. Beaded sign. Ultrasound signs of Caroli’s disease (red circle)
图2. 串珠征。Caroli病超声征象(红圈)
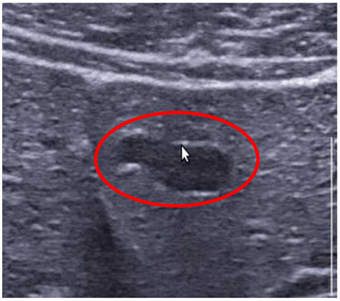
Figure 3. Intrahepatic cystic lesions were observed with a high frequency linear array probe in conjunction with the intrahepatic bile duct. Ultrasound signs of Caroli’s disease (red circle)
图3. 高频线阵探头观察到肝内囊性病变与肝内胆管相连续。Caroli病超声征象(红圈)
Table 2. Ultrasonographic findings of 15 patients with Caroli’s disease
表2. 15例Caroli病患者超声表现
3.3. 其他超声诊断
11例可见肝内胆管管形/树枝状扩张,3例可见肝外胆管管形扩张,3例合并胆囊结石,2例合并肝内胆管结石,9例合并肝弥漫性病变,2例合并海绵肾(见表2)。
4. 讨论
CD是一种以非阻塞性肝内胆管扩张为特征性表现的先天性疾病,发病率约1/100万,法国学者Caroli于1958年首次报道并描述本病 [1] 。CD发病机制尚未阐明,目前较为公认的假说为胚胎发育过程中肝内胆管在不同节段发生胆管板重塑异常。该病无性别差异,好发于儿童和青少年,多数人在30岁以前发病 [6] 。根据有无门静脉高压和肝内纤维化,将CD分为两种类型 [3] [4] :I型为单纯型,以肝内大胆管节段性扩张为特征,不伴先天性肝纤维化和门脉高压,常伴有胆囊炎、肝内胆管结石、胆囊结石等 [5] [7] ;II型为复杂型,较常见,在肝内胆管扩张的基础上,同时伴先天性肝纤维化、门脉高压及多囊性肾病,又称Caroli综合征 [8] [9] 。
肝活组织检查是诊断CD的金指标,但属于有创检查,影像学诊断往往是临床诊断CD最常用的方法。典型的增强CT图像表现为囊状扩张的胆管内见小圆点软组织密度影,增强后明显强化,称为“中心圆点征”,敏感度为71.4% [10] [11] 。MRCP是诊断本病最敏感的无创影像学方法 [12] [13] ,能全面清晰地显示整个胆管树,明确囊腔与胆管树相通情况。
超声在诊断CD方面的研究较少,且多为病例报道 [14] [15] [16] ,“中心圆点征”和“桥征”被认为是超声诊断本病的主要征象 [17] ,但目前未见上述征象在CD超声诊断效能方面的报道。本研究发现应用“中心圆点征”和“桥征”作为诊断征象的诊断符合率均为33.3%,且均在较大肝内囊性病变内出现这些征象,提示在肝内胆管重度囊性扩张的患者中更容易观察到“中心圆点征”和“桥征”,由于上述征象形成的病理基础为门静脉分支血管被周围扩张胆管包绕,“中心圆点征”和“桥征”是对被包绕的门脉血管的横切面和纵切面扫查,胆管扩张越严重,包绕门脉越明显,出现“中心圆点征”和“桥征”的可能性也就越大。反之,轻度胆管囊性扩张的患者,胆管没有形成对门脉的明显包绕,出现上述征象的可能性很小,这也是本研究“中心圆点征”和“桥征”多出现在较大的肝内胆管囊性扩张的病例中且同时出现的原因。由于本病形态上表现为肝内大胆管节段性囊性扩张,相应地,在影像上形成了“串珠征”和“囊尾征”,故观察到肝内囊性病变与肝内胆管相连续也就成为了本病最主要的影像学诊断依据,而囊性病变之间未发生病变的肝内胆管、尤其是内径较细的肝内胆管应用腹部低频探头观察较困难,且多个扩张的胆管往往不在同一平面上,导致“串珠征”和“囊尾征”的显示率仅为26.7%、46.7%。而高频探头明显改善了超声对肝内胆管的分辨能力,可以较好地显示扩张胆管和正常胆管的延续性,本研究中,高频超声模式下应用肝内囊性病变与肝内胆管相连续作为诊断指标,CD的超声诊断符合率达到了73.3%,与增强CT的诊断效能相当 [10] [11] ,是诊断CD较好的超声征象。另外,应用高频超声可以观察细小门脉的彩色血流和频谱,并以此识别相邻细小的肝内胆管,这也是高频超声在CD影像学诊断方面的独特优势。
本研究的局限性:应用高频线阵探头扫查存在的共性问题就是探查深度有限,本研究中1例患者因肝内囊性病变位于声像图远场,高频探头无法探及;对于胆管囊性病变范围较小、低频探头扫查仅表现为肝内胆管扩张或者囊性病变位于声像图不易显示区域的病例,即使应用高频探头诊断CD也是十分困难的,这也是本研究局限性所在。
NOTES
*通讯作者Email: zhaochengdr@163.com