摘要: 目的:探讨膝关节镜手术联合富血小板血浆治疗膝骨关节炎的临床疗效,并对制取时期不同所产生的影响进行探究。方法:回顾分析自2021年8月至2022年4月就诊于我院并行膝关节镜手术联合富血小板血浆治疗的膝骨关节炎患者60例,并根据制取时期分为实验组(术前制取PRP,共34例)和对照组(术后制取PRP,共26例),对比患者治疗后在视觉模拟量表(Vas)评分、Womac评分以及Lysholm评分的变化评估患者症状改变。结果:治疗后患者的Vas评分、Womac评分以及Lysholm评分均较治疗前有明显改善,且评分改变有统计学意义(P < 0.05);两组治疗前与治疗后各项评分的变化程度对比无明显差异(P > 0.05);术后两组患者均出现不同程度的血液炎性因子升高,在实验组中患者未出现任何特殊不良反应,而在对照组中我们发现有2例患者出现膝关节肿痛的现象,但该现象与术后患者自身炎性因子改变无明显相关性(P > 0.05)。结论:关节镜手术联合富血小板血浆能够缓解患者膝关节疼痛,改善膝关节功能,其中实验组末次随访评分展现出了较好的结果,但差异无统计学意义。
Abstract:
Objective: To investigate the therapeutic effect of knee arthroscopic surgery combined with plate-let-rich plasma in the treatment of knee osteoarthritis, and to explore the effects of different pro-duction periods. Methods: A retrospective analysis was conducted on 60 patients with knee osteo-arthritis who underwent knee arthroscopic surgery combined with platelet rich plasma treatment at our hospital from August 2021 to April 2022. They were divided into an experimental group (34 patients were treated with preoperative PRP) and a control group (26 patients were treated with postoperative PRP) based on the preparation period. The changes in visual analogue scale (Vas) score, Womac score, and Lysholm score were compared to evaluate the symptoms of the patients after treatment. Results: After treatment, the Vas score, Womac score, and Lysholm score of the pa-tients showed significant improvement compared to before treatment, and the changes in scores were statistically significant (P < 0.05); there was no significant difference in the degree of changes in various scores between the two groups before and after treatment (P > 0.05); After surgery, both groups of patients showed varying degrees of elevated blood inflammatory factors. In the experi-mental group, patients did not experience any special adverse reactions, while in the control group, we found 2 patients with knee joint swelling and pain. However, this phenomenon was not signifi-cantly correlated with postoperative changes in patients’ own inflammatory factors (P > 0.05). Con-clusion: Arthroscopic surgery combined with platelet rich plasma can alleviate knee pain and im-prove knee function in patients. The experimental group showed good results in the last follow-up score, but the difference was not statistically significant.
1. 引言
膝关节骨性关节炎(Knee osteoarthritis, KOA)是以老年人为主体,膝关节软骨缺损、软骨下骨改变以及滑膜组织炎症为主要特征的常见的膝关节退行性疾病 [1] ,其主要症状为疼痛、功能丧失、畸形等 [2] ,对患者的生活质量有严重的影响。目前的手术治疗方案主要为终末期的全膝关节置换手术以及中早期的膝关节镜手术。
富血小板血浆(platelet rich plasma, PRP)是一种从自身静脉血中通过离心的方式提取到的富含血小板的血浆,研究表明血小板激活后释放的生长因子(血小板衍生生长因子、转化生长因子、血管内皮生长因子、表皮生长因子等)对于膝关节软骨的修复有着促进作用 [3] [4] [5] ,相较于临床常用的透明质酸等药物,提纯自患者本身血液的PRP有副作用小、效果持续时间较长的优点,并且Sanchez等人的研究发现PRP能够显著延长患者行膝关节置换手术的时期 [6] 。随着科技发展,PRP提纯技术的发展使得PRP治疗再次被大众所关注,使其被广泛应用于KOA等疾病中 [7] ,而其多种的应用方案以及制取方式也引起了广大学者的争议 [8] 。
膝关节镜手术联合PRP是目前临床常见的治疗方案,有研究证明两种治疗方案的联合能够更好地促进术后患者疼痛的缓解以及功能的改善 [9] - [16] ,但对于联合两种治疗方案所取得的疗效仍存在争议并且目前联合治疗时PRP的制取时间、使用时机以及使用方式均没有获得共识,但有研究表明,PRP会因制取时如手术等外界因素使患者本身生理情况发生变化而受到影响 [17] 。本研究回顾性分析新疆维吾尔自治区人民医院骨科关节老年病区收治的行膝关节镜手术联合PRP治疗的患者,对患者治疗前后的疼痛评分(VAS评分)、Lysholm膝关节功能评分以及Womac评分进行比较,患者中包括:① 实验组:于术前采血制取PRP后在关节镜手术中行注射治疗;② 对照组:在关节镜手术术后24小时制取PRP并行注射治疗。本研究将对两组患者治疗前后的评分进行对比分析,为联合治疗的方案以及PRP的制取时期选择提供参考。
2. 资料与方法
2.1. 临床资料
本研究回顾性分析自2021年8月至2022年4月以来我院行膝关节镜手术联合PRP治疗患者86例,其中共60例完成随访,患者年龄分布为29~78岁,平均(49.05 ± 11.02)岁,患者血小板计数平均为(265 ± 63.75 × 109/L),均未出现血小板减低的情况,其中有26例因为患者个人原因选择术后第2天进行PRP关节腔灌注治疗,因此本文中将PRP术前制取术中使用视为实验组共34例,包括男11例,女23例;PRP术后制取注射治疗视为对照组共26例,包括男9例,女17例。组间一般资料比较均无统计学意义,见表1。本研究方案已经本院医学伦理委员会批准,所有参与患者及家属均知情同意。

Table 1. Comparison of general data between the two groups
表1. 两组间一般资料比较
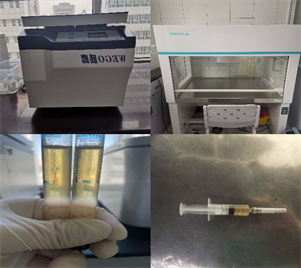
Figure 1. PRP workshop and finished PRP
图1. PRP工作间及成品PRP
2.2. PRP制取方法
使用采血针与注射器从患者静脉抽取所需血液后注入到离心管内,于离心机中配平离心后抽取最下层红细胞至分界面下3 mm~5 mm后弃除,将剩下部分摇匀后进行再次离心,离心结束再次抽取3/4上清液弃除后完成PRP制取,将试管内PRP用注射器取出备用(图1)。
2.3. 围手术期管理
患者入院后完善相关术前检查,术前有膝关节肿胀的患者行膝关节穿刺并培养排除感染性膝关节疾病,确保患者无明显异常检查结果后安排手术,根据分组制定PRP制取时间及手术方式。
2.4. 手术方法
所有手术均由有着丰富经验的主任医师进行,患者采用气管插管全身麻醉,入镜子后评估患者膝关节内滑膜、软骨、韧带等情况后进行对症清理或修整,韧带受损严重的患者予以排除,随后按不同分组进行不同的处理方案:
实验组:患者手术关节腔清理满意后使用生理盐水多次清洗关节腔,使用注射器将术前制备的PRP注入损伤清理部位后缝合切口(图2),使用弹力绷带加压包裹术区。
对照组:患者术后当天保持弹力绷带加压包裹,术后24小时将当天制取的PRP使用注射器注入患肢关节腔内进行关节腔灌注治疗。
2.5. 纳入排除标准
纳入标准:① 符合KOA诊断标准;② 无明显手术禁忌症;③ 非感染性疾病或风湿类疾病导致的膝关节损伤;④ 国际软骨修复协会软骨损伤分级系统(ICRS)分级I~II级者;⑤ 完整的随访资料且随访时间在3个月以上。
排除标准:① 患者K-L分级为IV级或III级或出现骨性畸形者;② 合并有血液系统疾病或Hb < 11 g/L以及血小板 < 1.5 × 109/L;③ 患有重要心脑血管疾病、肝肾功能不全、肿瘤晚期、系统性自身免疫病、或控制不佳的糖尿病患者;④ 1周内服用过非甾体类抗炎药(NSAIDs)、抗凝药或抗血小板药物者;⑤ 韧带损伤伴有关节不稳的患者;⑥ 体重指数(BMI) > 33者;⑦ 膝关节或肢体严重畸形者;⑧ 近6个月曾进行过关节内注射透明质酸治疗者;⑨ 依从性差难以配合者。
2.6. 评价标准
对患者进行Lysholm膝关节功能评分、膝关节WOMAC评分以及VAS疼痛评分并对两组治疗前后评分进行比较。通过比较,两组治疗前评分差异无统计学意义,见表2。
Table 2. Comparison of scores between the two groups before treatment
表2. 治疗前两组间各项评分比较
注:*采用t检验;#采用秩和检验。
2.7. 统计学方法
使用SPSS 24.0统计学软件进行分析,人数、年龄、各评分结果等定量资料满足正态分布的以均数 ±标准差表示,采用两独立样本t检验;偏态分布的则以中位数(四分位数间距)表示,采用Wilcoxon秩和检验;性别差异等定性资料采用χ2检验;检验水平设定为α = 0.05,P < 0.05为差异有统计学意义。
3. 结果
3.1. 评分结果
本研究患者均经过1~6个月的随访,患者治疗后末次随访的各项评分与治疗前评分的对比证明患者症状对比治疗前均有好转(P < 0.05),见表3。
Table 3. Comparison of scores of all patients before and after treatment
表3. 全部患者治疗前后各项评分对比
通过对治疗前后的评分进行对比可以看出在两个不同时期制取PRP并进行治疗后,患者在末次随访时症状均出现了改善(P < 0.05,见表4),但两组间各项评分比较均无统计学意义(P > 0.05),见表5。
Table 4. Comparison of the scores before and after treatment between the two groups
表4. 两组患者治疗前后各项评分对比
Table 5. Comparison of changes in scores between the two groups
表5. 两组评分变化程度对比
3.2. 安全性结果
本研究中患者术后C-反应蛋白(C-reactive protein, CRP)均未见异常,而部分患者术后有不同程度的中性粒细胞百分比(granulocyte, GR%)增高(见表6),且患者经随访调查发现,实验组患者均未出现红肿、胀痛等症状,但在对照组患者的随访中发现有2例患者出现了3天内的膝关节肿痛,虽然差异无统计学意义(P > 0.05),且与患者炎性因子升高未发现明显相关性,但有可能因样本量较少而产生误差有关。
Table 6. Data of postoperative serum inflammatory factors in two groups
表6. 两组术后血清炎性因子资料
4. 讨论
KOA是关节炎中最为常见的类型,与个人年龄以及体重等因素密切相关,有研究表明60岁以上的人群中约有10%的男性以及13%的女性患有KOA,而当年纪达到70岁后,这一比例更是会突增到40%,通过研究,Magnusson K等人认为患者中女性患者要比男性患者更多 [18] ,本研究数据与这一观点相吻合。而随着国内人口老龄化的发展,KOA的发病率居高不下,如果不及时进行治疗干预,不仅会导致患者病情的进展,还会对患者的身心健康造成影响。
关节镜手术联合PRP治疗已经成为了一种在临床常见的治疗中早期KOA的诊疗方案,有研究表明关节镜手术可以改善中度或重度KOA患者的膝关节功能以及活动能力,尤其是伴有半月板或软骨病变的患者 [19] [20] ,而PRP关节腔注射治疗有研究发现能够改善关节软骨缺损的情况 [21] [22] [23] 。理论上讲,两种治疗联合不但能达到关节镜手术冲洗炎性因子,清理关节腔内软骨碎片等磨损因素的目的,还能达到PRP注射治疗恢复软骨缺损的目标。但目前关于PRP使用的研究差异性大,包括制取方式、制取时间、使用方式等,缺少足够高质量的证据以及指南。
本研究中术后患者因自身应激反应导致有部分患者出现了GR%的升高,而通过治疗前后评分对比可以得出结论:患者在经过治疗后膝关节功能以及疼痛情况均出现了明显好转,从随访末期的评分结果可以发现两组末次随访评分均得到了明显改善,证明了两组的治疗方案对于中早期膝骨关节炎有着良好的疗效,但在两组间的评分对比中未发现明显的差距(P > 0.05)。值得注意的是在对照组中我们发现了2例术后持续时间在3天内的膝关节肿痛情况,虽然与实验组之间的差异无统计学意义(P > 0.05),且与患者血清炎性因子的变化之间也并未发现明显的相关性,但有可能是样本量较低导致误差的产生,因此我们认为患者术后制取的PRP有导致患者膝关节肿痛的趋势,并且可能与自身术后某些炎性因子的增加有关。
本研究的不足之处:未能获取患者手术前后多项血清炎性因子的详细资料,因此无法进行进一步的对比研究。本研究未能获取患者的详细影像学资料,无法对患者如膝关节软骨等改变进行对比分析。
综上所述,关节镜手术联合PRP治疗能够缓解KOA患者疼痛,改善膝关节功能,术中注射PRP治疗能够避免患者术后遭受二次损伤,减轻患者遭受的痛苦,因此笔者认为应该尽可能采用该种治疗方案,但本研究中PRP的制取与注射治疗时期并未对长期疗效产生明显的影响,因此可根据情况灵活选择适宜的治疗计划,但选择在术后制取PRP并进行注射治疗时需注意可能导致患者出现短期膝关节肿痛的可能性。
NOTES
*通讯作者。