1. 引言
前交叉韧带(anterior cruciate ligament, ACL)损伤可以通过接触性或非接触性机制发生。其中非接触性机制是最常见的,被归类为在改变方向或着陆运动时突然减速导致的韧带断裂 [1] [2] 。接触性机制通常是直接作用于膝关节外侧的力使其外翻而发生的韧带断裂 [2] 。对非接触性损伤机制的准确推断,这对于了解ACL损伤危险因素和制定有效的预防策略是必不可少的 [2] [3] [4] 。
在前交叉韧带损伤过程中,较大的外力导致股骨和胫骨之间发生剧烈撞击,力量转移到软骨下骨,骨小梁损伤后发生出血、水肿,形成骨挫伤 [1] [5] [6] ,见于80%~99%的急性ACL损伤 [2] [5] [6] 。这些隐匿性骨损伤可以清晰的在磁共振成像(MRI)扫描中被发现,在脂肪抑制T2加权图像上表现为软骨下的高信号,称为骨髓水肿或水肿样骨髓信号强度 [7] 。膝关节骨挫伤的分布代表了ACL损伤时股骨和胫骨发生碰撞性损伤的位置,通过评估骨挫伤模式可以更深入的了解ACL损伤机制 [5] [8] [9] 。
Patel等人 [8] 在ACL损伤后MRI采集期的研究中,其所有纳入的研究中,MRI采集期从6天到9周不等。Graf等人 [10] 研究发现,他们的ACL损伤患者的骨挫伤在损伤后大约6周就消失了。Tung等人 [11] 的报道中,他们的受试者在最初损伤后平均4.3周接受了MRI检查。由于骨挫伤可能在一段时间后消退,为了准确的将骨挫伤模式与损伤机制联系起来,在受伤后30内进行MRI检查是本研究获得最准确数据的严格纳入标准。
如何来准确、可靠的描述急性ACL损伤膝关节内骨挫伤的模式,目前公认的标测方法有限。本研究的目的是采用Jay Moran等人 [2] 提出的一种新的标测技术,来更可靠的描述非接触性前交叉韧带(ACL)损伤的骨挫伤模式,并进一步来验证文献中最常见的ACL损伤的机制,包括外翻应力、胫骨前平移和胫骨内旋转。
2. 方法
2.1. 研究对象
在2021~2023年期间,查找出数百名患者于青岛大学附属医院关节外科及运动医学科接受前交叉韧带重建手术,其中100名患者符合本研究的以下纳入标准:(1) 损伤日期和MRI检查日期之间 < 30天;(2) 在冠状位和矢状位均有脂肪抑制T2加权图像的MRI序列;(3) 损伤机制有记录;(4) 非接触性前交叉韧带损伤;(5) 没有前交叉韧带损伤既往史;(6) 单纯前交叉韧带损伤,无伴随的后交叉韧带及内、外侧副韧带损伤。
2.2. 研究方法
根据病历中患者对受伤过程的描述,损伤机制被记录为非接触性或接触性。同时记录患者的性别、年龄、BMI、损伤日期和MRI检查日期。所有100名患者均在本院3.0TMR仪器上按标准膝关节操作规程进行了膝关节MRI检查。所有影像学研究均由同一名有丰富经验的医师进行回顾性审查,记录脂肪抑制T2加权冠状位和矢状位图像中骨髓水肿的位置。
2.3. 骨髓水肿定位
本研究中采用的标测技术,在描述骨髓水肿位置这方面,区域数量更多,定位更明确。以下分别在冠状位及矢状位对病变位置进行分区。
2.3.1. 冠状位
在冠状位股骨和胫骨的分区如图1。
通过股骨髁间切迹中央的一条线(红线)将股骨和胫骨分为内侧和外侧,分别记录为股骨内侧髁(medial femoral condyle, MFC)、股骨外侧髁(lateral femoral condyle, LFC)、胫骨内侧平台(medial tibial plateau, MTP)与胫骨外侧平台(lateral tibial plateau, LTP)。其中内侧、外侧半月板的外周和内侧游离边缘(蓝线)之间的区域,分别记录为股骨内髁内侧(femoral-medial-medial, FMM)、股骨外髁外侧(femoral-lateral-lateral, FLL)、胫骨内侧平台内侧(tibia-medial-medial, TMM)和胫骨外侧平台外侧(tibia-lateral-lateral, TLL)。

Figure 1. Femoral and tibial zones in the coronal plane
图1. 股骨、胫骨冠状位分区
更中央部经过胫骨内、外侧髁间棘的斜坡起点处的一条线(黄线)将中央部进一步细分。图中蓝线和黄线之间的区域分别为:股骨内侧髁中央(femoral-medial-central, FMC)、股骨外侧髁中央(femoral-lateral-central, FLC)、胫骨内侧平台中央(tibia-medial-central, TMC)和胫骨外侧平台中央(tibia-lateral-central, TLC)。图中黄线与正中线(红线)之间的区域分别记录为:股骨髁间切迹内侧(femoral-medial-notch, FMN)、股骨髁间切迹外侧(femoral-lateral-notch, FLN)、胫骨内侧棘下区(tibia-medial-subspine, TMS)和胫骨外侧棘下区(tibia-lateral-subspine, TLS)。
在冠状面上以髁间切迹为界,其近端被正中线分为:股骨滑车内侧(femoral-medial-trochlea, FMT)和股骨滑车外侧(femoral-lateral-trochlea, FLT)。
2.3.2. 矢状位
记录冠状位的位置后,采用矢状位描述病变位置在股骨和胫骨的前后位置(如图2、图3)。
股骨区将股骨内、外侧髁分为滑车区域(T)、中央部(C)和后部(P)。股骨的矢状位标志首先将每个股骨髁关节软骨的最近端相连,其连线(白线)的中点(白色五角星)被认为是股骨矢状位的中心轴,从该点延伸到胫骨平台最前(红线)和最后(蓝线)的线将股骨髁分为T、C和P。从中心轴延伸到股骨和胫骨关节软骨接触区域的最前侧的一条线(黄线),将股骨中央部进一步细分出前中央部(A)。
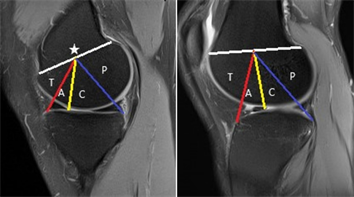
Figure 2. Femoral and tibial zones in the sagittal plane
图2. 股骨矢状位分区
胫骨区将胫骨内、外侧平台分为3个区域:前部(A)、中央部(C)和后部(P)。其分界线经过股骨和胫骨关节软骨接触区域的最前侧(红线)以及每个半月板后角游离边缘的最前侧(黄线)。
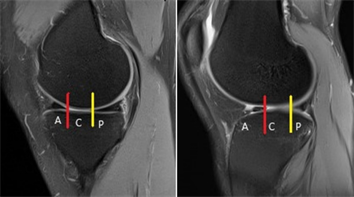
Figure 3. Tibial zones in the sagittal plane
图3. 胫骨矢状位分区
2.4. 数据收集
记录患者的性别、年龄、BMI、损伤日期和MRI检查日期。
记录每位患者在冠状位及矢状位的骨髓水肿位置。如果病灶位于多个区域,则对其延伸到的每个单独区域进行计数。如果单个区域内存在多个病灶,则只计数其所跨越的单个区域。并不记录骨髓水肿的信号强度和体积。
对相同的数据集进行两次回顾性审查,两侧次审查之间的时间间隔为6周。
2.5. 统计学分析
计量数据采用(
),使用组内相关系数(ICCs)评估两次骨挫伤位置记录的可靠性。ICC值解释如下:<0.5差,0.5至0.75中等,0.75至0.9良好,>0.90优秀。对骨挫伤模式的分析,使用卡方检验来分析研究队列中骨挫伤频率,以描述损伤的机制。所有统计数据均使用SPSS统计学软件进行分析。有意义的阈值设定为P < 0.05。
3. 结果
在我们的研究队列中,年龄平均值为29.66 ± 9.65岁,男性与女性比例为76/24,BMI平均值为25.05 ± 3.73,损伤时间和MRI检查时间之间平均为9.59天。
对相同数据集的两次回顾性审查过程中,记录股骨侧病灶位置时,两次记录间的ICC值分别为0.983,胫骨侧的ICC值为0.986,所有ICC值均表明描述ACL损伤中骨髓水肿位置的可靠性极高。
综合全部的数据,有86%患者至少有1处骨髓水肿。其中47%的膝关节(n = 47)在MFC至少有1个病变,60%的膝关节(n = 60)在LFC至少有1个病变,这些差异无统计学意义(P > 0.05)。同样,MTP与LTP至少有1个病变的膝关节数量分别为44、79,这没有统计学显著性差异(44% vs 79%; P > 0.05)。
在评估冠状面总病灶数时,发现股骨外侧髁相对于内侧髁病灶更多(221 vs 83; P < 0.001),同样在胫骨平台处,与内侧平台相比,外侧平台的病灶数更多(254 vs 97; P < 0.001) (如表1) 。

Table 1. The total bone lesions in the medial and lateral compartment zones for the femur and tibia
表1. 股骨、胫骨内外侧间室病灶分布
在矢状面,股骨的病灶几乎完全位于股骨髁的前部/中央部区域(286; 94.1%),而不是后部区域(18; 5.9%)。与之相反的是,胫骨的病灶局限于两个平台的后部区域(263; 74.9%),而不是前部/中央区域(88; 25.1%) (如表2)。
Table 2. The total bone lesions at the femur and tibia in the anterior/central and posterior zones
表2. 股骨胫骨前/中部及后部病灶分布
结合冠状位及矢状位对股骨侧病灶位置的进行分析,发现股骨外侧病灶多位于FLL前部(40%)及FLC前部(12%),而在股骨内侧病灶多位于FMM中央部(如表3)。
Table 3. The bone lesions at the femur
表3. 股骨侧的病灶分布
在胫骨平台病灶的研究中,发现病灶部位明显局限于两侧胫骨平台的后部区域。胫骨内侧平台后部由内到外分别是TMM后部30%、TMC后部29%以及TMS后部23%,胫骨外侧平台后部由内到外分别是TLS后部43%、TLC后部71%以及TLL后部67% (如表4)。
Table 4. The bone lesions at the tibia
表4. 胫骨侧的病灶分布
4. 讨论
目前公认的对骨挫伤模式的标测技术有限,Patel等人 [8] 对前交叉韧带损伤的骨挫伤模式进行了系统评价,并指出很少有研究一致、准确地报告了挫伤的位置。大多数研究将水肿局限于LFC、LTP、MFC或MTP,没有进一步描述在各个股骨髁和胫骨平台的具体位置 [5] [8] [12] 。本文是根据Jay Moran等人 [2] 研究的一种新的标测技术,其结合了国际软骨修复学会(ICRS)的胫股关节软骨手术病变图 [13] 以及全器官磁共振成像评分(WORMS)映射系统 [14] ,这两种系统在评估骨关节炎中膝关节软骨病变、半月板撕裂和骨髓病变具有出色的可靠性。Peterfy等人 [14] 的对WORMS评分的研究中,在冠状位将股骨和胫骨分为内侧和外侧两个间室,将胫骨额外添加一个胫骨棘区域,矢状位将股骨和胫骨分为前、中、后三部分,其观察者间对WORMS评分的一致性很高(大多数ICC值为 > 0.80)。与WORMS相比,ICRS方法在冠状位具有更多区域,并且国际软骨研究学会承认了这种膝关节病变定位的精确性问题 [13] [15] 。本研究进一步将股骨远端冠状位分为8个区,矢状位分为4个区,将胫骨近端在冠状位和矢状位分别分为6个区和4个区。冠状位的进一步分区并与矢状位从前到后的位置相结合,可以更精准的对骨挫伤模式进行描述 [16] 。
采用这种新的标测技术对相同数据集的两次回顾性审查中,所有ICC值均 > 0.9,这表明其用来描述非接触性前交叉韧带损伤中骨髓水肿位置的可靠性极高。急性ACL损伤膝关节骨髓水肿精准定位有助于进一步阐明损伤机制。
本研究中确定的骨挫伤模式与文献中报道的非接触性前交叉韧带损伤的机制相一致,进一步支持了这种新的标测技术的使用。我们发现,与膝关节胫股内侧间室相比,膝关节胫股外侧间室内的骨挫伤明显更多,这表明在ACL损伤时,LFC和LTP之间的碰撞比MFC和MTP之间的碰撞更剧烈,与先前文献报道的ACL损伤骨挫伤模式的研究结果一致 [5] [8] [12] [17] [18] [19] 。这种骨挫伤模式归因于损伤期间膝关节的外翻应力,导致股骨和胫骨的外侧受压,与胫股内侧间室相比,胫股外侧间室内的碰撞更强烈。
通过矢状面分析,我们发现两个股骨髁上的骨挫伤局限于前部和中央部,而两个胫骨平台上的骨挫伤局限于后部区域 [20] 。这些发现表明,在损伤过程中,双侧胫骨平台的后部区域与内、外侧股骨髁的前/中央部相碰撞,这需要胫骨后部在内侧和外侧都必须相对于股骨向前平移,这种矢状面骨挫伤模式与先前研究报告的胫骨前平移相吻合 [5] [8] [12] [19] [21] [22] 。
研究MFC和LFC上矢状面骨挫伤模式的不同有助于了解胫骨内旋或外旋的程度。我们发现LFC上骨挫伤局限于前部,而在MFC上观察到的骨挫伤局限于中央区域。在单纯胫骨前平移且没有胫骨内外旋转的情况下,MFC和LFC上的矢状面骨挫伤模式位于相同的矢状面区域。而当胫骨内旋转时,LTP的后部区域向前旋转,MTP的后部区域向后旋转,导致LTP后部与LFC的碰撞比MTP后部与MFC的碰撞更靠前,这与我们发现的骨挫伤模式一致,同时之前研究报道ACL损伤时伴随着胫骨的旋转这一结论相符合 [5] [8] [12] 。
本研究中确定的骨挫伤模式表明,在非接触性前交叉韧带损伤中,胫骨内旋时发生外翻和前平移,这些结果与先前的研究相一致,进一步支持了这种新的标测技术的使用 [12] [23] [24] 。
5. 结论
新的标测为描述非接触性ACL损伤中的骨挫伤模式提供了一种标准化且可靠的方法,使用该技术确定的骨挫伤模式表明了非接触性ACL损伤最常见的机制:外翻应力、胫骨前平移和胫骨内旋转。
致 谢
感谢王英振教授、项帅博士对文章的指导并提出修改建议。
NOTES
*通讯作者。